
Wavelength is the single most important variable in light therapy, also known as photobiomodulation (PBM). It determines which biological structures absorb light, how deep that light travels into tissue, and which cellular repair processes switch on. The role of wavelength in light therapy is not cosmetic. Blue light at 405–420 nm targets bacteria in acne-prone skin. Red light at 625–660 nm stimulates collagen-producing fibroblasts. Near-infrared (NIR) light at 700–850 nm reaches muscles, tendons, and deeper dermal layers. Choose the wrong wavelength and the light simply does not reach its target. Choose the right one and you trigger measurable biochemical change.
How does wavelength affect light therapy outcomes?
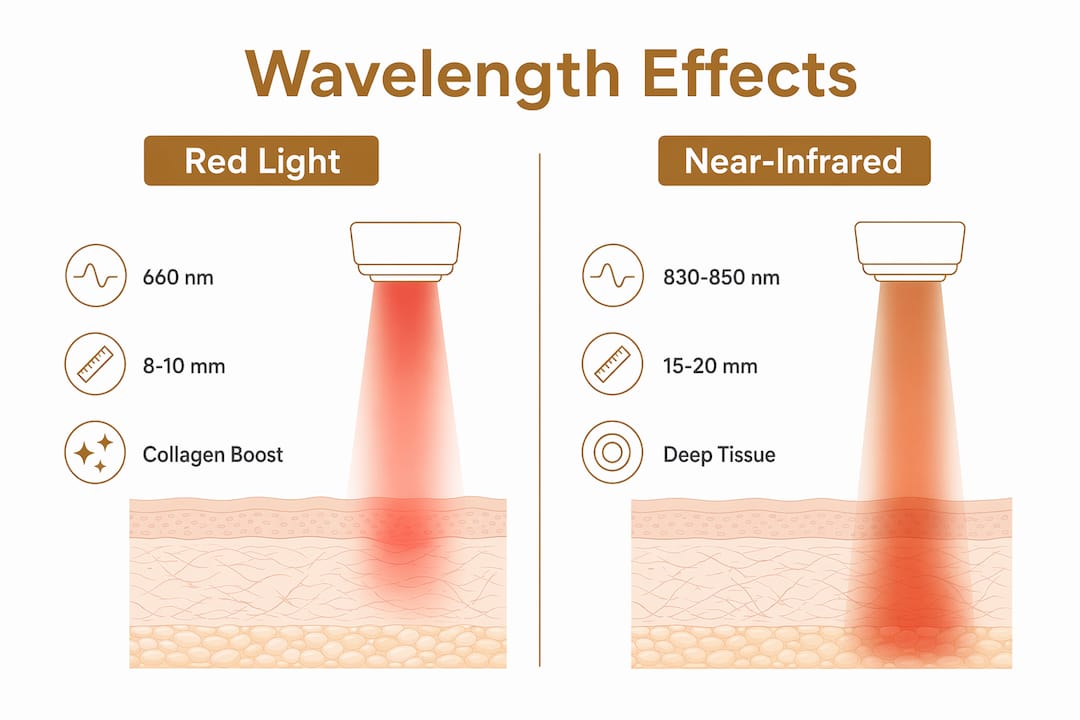
Wavelength determines which chromophores inside your cells absorb light energy. A chromophore is a molecule that captures photons and converts them into a biological signal. The most studied chromophore in PBM is cytochrome c oxidase (CCO), an enzyme inside the mitochondria. CCO has absorption peaks at around 660 nm (red) and 810–850 nm (NIR). When light hits those peaks, CCO triggers ATP production, nitric oxide release, and inflammation modulation. Miss those peaks and the photons pass through or scatter without effect.
Penetration depth follows directly from wavelength. Red light at 660 nm penetrates roughly 8–10 mm into skin, reaching the dermis where collagen lives. NIR at 850 nm penetrates 40–50 mm, reaching muscle tissue, tendons, and joint structures. That difference is not trivial. A device emitting only red light cannot treat a deep shoulder injury, just as a NIR-only device is less suited to surface-level acne treatment.

Red and NIR wavelengths also activate distinct signalling pathways. Red and NIR light promote the PI3K/Akt/mTOR pathway, which drives anabolic tissue repair. Blue light engages different molecular targets, producing secretory and antimicrobial effects. Think of each wavelength as a different key. Each one opens a different biological door.
What are the effects of different wavelengths on skin and healing?
Each wavelength band produces specific, well-documented effects on skin and tissue. Understanding these effects helps you match the right light to the right goal.
- Blue light (405–420 nm): Targets porphyrins, compounds produced by Cutibacterium acnes bacteria. When blue light hits porphyrins, it generates reactive oxygen species that destroy the bacteria. This makes blue light the primary wavelength for acne treatment. It does not penetrate deeply, so its benefits are confined to the skin surface.
- Red light (625–660 nm): Stimulates fibroblasts in the dermis to produce collagen and elastin. Clinical protocols commonly use 633 nm or 660 nm for skin texture improvement, fine line reduction, and wound healing. This is the workhorse wavelength for at-home anti-aging treatments.
- Near-infrared (700–850 nm): Reaches deeper tissues to modulate inflammation, accelerate muscle recovery, and support joint health. NIR is less visible to the eye but more penetrating than red light. It is the preferred wavelength for musculoskeletal conditions and deeper dermal remodelling.
- Combined red and NIR: Combining 633 or 660 nm red with 830 or 850 nm NIR produces greater improvements in skin texture and fine lines than either wavelength alone. Red handles superficial collagen stimulation; NIR manages deeper inflammation. Together, they address multiple skin layers simultaneously.
Pro Tip: If your primary goal is anti-aging, look for a device that emits both red (around 660 nm) and NIR (around 830–850 nm). Single-wavelength red devices work, but the dual-wavelength combination delivers faster and broader results.
Why does matching wavelength to tissue depth matter?
Selecting the wrong wavelength for your treatment goal is one of the most common and costly errors in light therapy. Tissue absorbs and scatters light differently depending on its composition. Skin, fat, muscle, and bone each have distinct optical properties. A wavelength that works brilliantly at the skin surface may scatter almost entirely before reaching a deeper target.
Here is a practical framework for matching wavelength to goal:
- Surface skin concerns (acne, redness, superficial pigmentation): Use blue (405–420 nm) or red (625–660 nm). These wavelengths interact with the epidermis and upper dermis without needing deep penetration.
- Collagen stimulation and fine lines: Red light at 660 nm is the primary choice. It reaches fibroblasts in the dermis and activates collagen synthesis directly. For choosing the right wavelength for your skin type, device specifications matter enormously.
- Deeper inflammation and muscle recovery: NIR at 810–850 nm is required. Red light simply does not travel far enough to reach inflamed tendons or deep muscle fibres.
- Comprehensive anti-aging: Combine red and NIR. This addresses both the dermis and the deeper tissue layers, producing synergistic collagen and repair benefits.
- Darker skin tones: Melanin absorbs red light more efficiently than NIR, which reduces effective penetration at 660 nm. People with darker skin tones may need longer session times at red wavelengths or a greater emphasis on NIR to achieve the same therapeutic dose at depth.
Skin pigmentation is a factor many device manufacturers do not address clearly. Melanin is a chromophore too, and it competes with CCO for red photons. NIR at 850 nm penetrates more uniformly across skin tones, making it a more consistent choice for deeper targets regardless of pigmentation.
Pro Tip: If you have a medium to deep skin tone, prioritise devices with a strong NIR output alongside red. You will achieve more consistent results at depth without needing to dramatically extend session times.
How do irradiance and energy dose shape wavelength effectiveness?
Wavelength alone does not determine results. Two other parameters are equally critical: irradiance and energy dose. Irradiance is the power delivered per unit area, measured in milliwatts per square centimetre (mW/cm²). Energy dose, or fluence, is the total energy delivered over a session, measured in joules per square centimetre (J/cm²).
Consumer LED devices typically deliver 5–35 mW/cm² and 1–5 J/cm² per session. Clinical photobiomodulation devices require 20–60 J/cm² for full efficacy. That gap explains why home devices produce gradual rather than immediate results. The wavelength may be correct, but the energy delivered is lower, so the cellular response builds more slowly over repeated sessions.
| Wavelength | Typical penetration depth | Recommended energy dose | Primary target |
|---|---|---|---|
| Blue (405–420 nm) | 1–2 mm | 1–4 J/cm² | Skin surface, bacteria |
| Red (625–660 nm) | 8–10 mm | 4–20 J/cm² | Dermis, fibroblasts, collagen |
| NIR (810–850 nm) | 40–50 mm | 10–60 J/cm² | Muscle, tendons, deep dermis |
The table above illustrates why a device with the right wavelength but insufficient irradiance still underperforms. A 660 nm LED emitting 5 mW/cm² will produce some collagen stimulation, but the effect accumulates slowly. Clinical results require either higher power or longer sessions to compensate.
Key points to understand about energy and protocol:
- Consistency matters more than intensity for home devices. Daily or every-other-day sessions over 8–12 weeks outperform sporadic high-intensity sessions.
- Session duration typically runs 10–20 minutes per area for consumer devices, compensating for lower irradiance.
- Multi-wavelength panels covering larger surface areas deliver more total energy per session than small handheld devices.
What are the most common misconceptions about wavelength in light therapy?
Several persistent myths lead people to buy ineffective devices or use them incorrectly. Correcting these saves time, money, and frustration.
- “Brighter means better.” NIR devices appear dimmer because 850 nm light is largely invisible to the human eye. A device glowing intensely red is not necessarily more therapeutic than one emitting a faint glow. Always check the wavelength and irradiance specifications, not the visual brightness.
- “More power always produces better results.” Photobiomodulation follows the Arndt-Schultz biphasic law: too little energy has no effect, but too much causes oxidative stress that inhibits healing. Overexposure is a real risk, particularly with high-powered clinical devices used without guidance.
- “One session is enough to see results.” Consumer devices require cumulative exposure. Cellular repair processes build over weeks, not hours. Expecting immediate results leads to abandoning effective protocols too early.
- “Any red light device treats the same conditions.” A device emitting 630 nm differs meaningfully from one emitting 660 nm. Both are “red,” but their absorption profiles and penetration depths differ. Specificity matters.
- “Wavelength is all that counts.” Effectiveness depends on wavelength and also irradiance and dosage. A perfectly matched wavelength at insufficient power produces weak results.
Pro Tip: Before purchasing any light therapy device, request the irradiance specification in mW/cm² at a stated distance. If a brand cannot provide this figure, treat that as a red flag about device quality.
How to choose a light therapy device based on wavelength
Selecting a device requires matching its specifications to your specific skin or wellness goals. The following criteria are worth evaluating before any purchase.
- Wavelength specification: Confirm the exact nanometre values. “Red light” is not sufficient. Look for 630–660 nm for skin and 810–850 nm for deeper targets.
- Irradiance output: Aim for at least 20 mW/cm² at the treatment distance for meaningful results with home devices.
- Multi-wavelength capability: Devices combining red and NIR wavelengths deliver broader benefits. For LED mask selection guidance, wavelength range is the first filter to apply.
- Treatment area coverage: Panels and masks cover more surface area per session than handheld wands, delivering more total energy efficiently.
- Session duration guidance: Reputable devices specify recommended session lengths. Follow them. Longer is not always better given the biphasic dose response.
- Skin tone considerations: If you have a deeper skin tone, prioritise devices with strong NIR output alongside red. Consult at-home skincare guidance for personalised protocol advice.
Realistic expectations matter. Consumer devices produce visible improvements in skin texture, fine lines, and tone over 8–12 weeks of consistent use. They are not equivalent to clinical sessions, but they deliver genuine benefit when used correctly and consistently.
Key takeaways
Wavelength is the foundational variable in light therapy: selecting the correct nanometre range for your target tissue determines whether treatment triggers genuine cellular repair or produces no effect at all.
| Point | Details |
|---|---|
| Wavelength determines penetration | Red (660 nm) reaches 8–10 mm; NIR (850 nm) reaches 40–50 mm into tissue. |
| Chromophore matching is critical | Cytochrome c oxidase absorbs at 660 nm and 810–850 nm, triggering ATP and repair. |
| Combine red and NIR for anti-aging | Dual-wavelength protocols outperform single-wavelength for collagen and inflammation. |
| Irradiance and dose complete the picture | Correct wavelength at insufficient power still produces weak results over time. |
| Skin tone affects dosing | Melanin competes for red photons; darker skin tones benefit from greater NIR emphasis. |
What I have learned from watching people use light therapy
Most people who are disappointed by light therapy made the same mistake: they bought a device based on how it looked rather than what it emitted. A bright, warm-glowing panel feels therapeutic. But if it emits 630 nm at 8 mW/cm², it is delivering a fraction of the energy needed to meaningfully stimulate collagen at dermal depth.
The science here is genuinely settled. Cytochrome c oxidase responds to specific wavelengths. The biphasic dose curve is real. Skin pigmentation affects penetration. These are not contested points. What surprises me is how rarely device brands communicate this clearly. Marketing copy leans on “red light” as a category rather than specifying the nanometre value and irradiance output that actually determine results.
The most promising development I have seen is the shift toward multi-wavelength devices that combine red and NIR in a single panel or mask. These address the limitation of single-wavelength tools by treating multiple tissue depths simultaneously. For anyone serious about skin rejuvenation or recovery, a dual-wavelength device is not a luxury. It is the logical minimum.
My honest advice: treat wavelength selection the way you treat SPF selection. The number matters. “Sunscreen” is not enough information. Neither is “red light.”
— Adam
Glowera’s light therapy devices for wavelength-specific skincare
Glowera stocks a curated range of LED light therapy devices covering blue, red, and near-infrared wavelengths, sourced from internationally recognised beauty tech brands and delivered across Saudi Arabia. Each device in the collection is selected for verified wavelength specifications and clinically relevant irradiance output, not just visual appeal.
Whether your goal is acne control with blue light, collagen stimulation with red, or deeper tissue recovery with NIR, Glowera’s range includes options across all three categories. Multi-wavelength masks combining red and NIR are available for those targeting anti-aging results at multiple skin depths. Browse the full LED skincare collection to find a device matched to your wavelength needs and skin goals.
FAQ
What wavelength is best for skin rejuvenation?
Red light at 630–660 nm is the primary wavelength for skin rejuvenation, stimulating fibroblasts to produce collagen and elastin in the dermis. Combining it with NIR at 830–850 nm produces greater improvements in skin texture and fine lines than red light alone.
How deep does red light penetrate compared to near-infrared?
Red light at 660 nm penetrates approximately 8–10 mm into skin, reaching the dermis. Near-infrared at 850 nm penetrates 40–50 mm, reaching muscle tissue and deeper joint structures.
Does skin tone affect light therapy results?
Yes. Melanin absorbs red light more efficiently than NIR, reducing penetration depth in darker skin tones. People with medium to deep skin tones may need longer sessions at red wavelengths or a stronger NIR component to achieve equivalent therapeutic dosing at depth.
Why does my NIR device look dim if it is working?
Near-infrared light at 850 nm sits largely outside the visible spectrum, so effective NIR devices appear dimmer than red light devices. Brightness is not a reliable indicator of therapeutic output. Always evaluate irradiance in mW/cm² rather than visual intensity.
How many sessions does light therapy require to show results?
Consumer devices typically require 8–12 weeks of consistent use, with sessions every day or every other day, before visible improvements in skin texture and fine lines become apparent. Lower irradiance output in home devices means results accumulate gradually rather than immediately.



